




 Turkish
Turkish Deutsch
DeutschShoulder Stuck of Fetus
Shoulder stuck refers to the difficulty in the delivery of the shoulders after the head is pushed out during vaginal delivery.
One shoulder or two shoulders can be stucked. The main reason is the discrepancy between the woman’s birth canal called pelvis and baby’s shoulder size.
It is not often predictable and predictable. But:
- in mothers with short height
- In the cases where the circumference of the baby is wide,
- In the obesity during pregnancy
- In the pregnancy diabetes
- in the cases of large fetus
- in fast delivery
- in multiple pregnancies
It is known that the frequency is increased in case of having to use tools such as vacuum and forceps at birth.
The most common risk factors are mother’s diabetes and large baby. However, 50-60% of the shoulder stuck is seen in babies under 4000 gr. However, it is generally encountered during the birth of pregnant women who are not at high risk.
Although cesarean is frequently applied to reduce the rate of shoulder stuck in large babies, it should be noted that 50% of the cases are below 4000 gr. reducing the frequency of permanent injury can also be a factor in the need for cesarean delivery. Abdominal circumference measurement and comparison of head circumference and abdominal circumference measurements can help in risk assessment.
Shoulder insertion frequency is given with a frequency ranging from 0.2% to 3%. The frequencies in the studies being so variable may be related to the risk factors of pregnancies. It should not be evaluated the normal weight baby and large baby or diabetic pregnant and non-diabetic pregnant with the same frequency.
If a shoulder is stucked, the following may develop in the mother:
* Postpartum haemorrhage (11%)
* Tearing of the uterus during childbirth
* Tears in the cervix and vagina (4%)
* The frequency of depression increases after birth
If a is stucked, the following may develop in the fetus:
* Brachial plexus palsy
* Baby’s lack of oxygen and cerebral palsy
* Baby’s loss may occur.
The most common is brachial plexus palsy which concerns the damage to the nerve roots caused by the trauma caused by the stuck of the shoulder of the fifth and sixth neck vertebrae. It is temporary in 90-95% of cases and heals completely. While it is thought that the application of excessive traction (pulling) on the baby’s head to remove the shoulder after the birth of the head is the cause of wearing the shoulder, today the tension formed in the pelvis when the shoulder is attached is known to stretch the brachial plexus and cause damage.
The increase in the obesity rate in the mother is also directly correlated to the increase in risk. Increasing the rate of large baby and diabetic pregnancy in obesity also contributes to this risk increase.
The probability of recurrence in the subsequent birth is given to 11-12% in women who have had a shoulder implant before, since cesarean is often preferred after problematic delivery experience, the actual frequency is not completely known.
In order to accurately estimate the fetal weight, besides fetal weight estimation made by ultrasonography, weight estimation should be supported by clinical measurement of the abdomen. When these two methods are used together, weight estimation can be made more accurately. It should be remembered that weight estimation by ultrasonography is 10% error margin.
The second phase of birth; When the baby’s passage through the birth canal and the cervix is fully opened, the phase containing the strain phase lasts more than 2 hours is a sign that the risk of wearing a shoulder in large babies will increase, and in this case vacuum etc. cesarean should be preferred instead of birth in the instrument such as donning. Conversely, getting out too fast is an important risk factor for shoulder stuck, and it is important that the team is prepared for it.
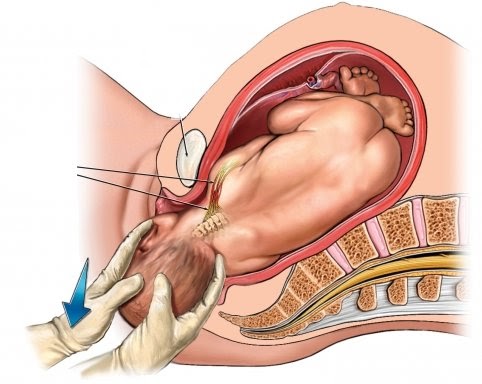
Managing the shoulder stuck is a team job. An anaesthesiologist, paediatrician, an experienced midwife, a second obstetrician are required. Once the shoulder is diagnosed, the strain is stopped and the woman’s hip is at the proper place on the birth table. The first preferred manoeuvre is the McRoberts manoeuvre. The legs of the mother are pulled from the side to the side and rest on the sides of the abdomen. Then, pressure is applied on the midline bone in front of the pelvis, which is called the pubis bone, and the birth of the front shoulder is facilitated. A combination of Mc Roberts and suprapubic pressure has been reported with a 58% success rate.
In cases where these two manoeuvres fail, rotation mechanisms are tried. It is planned to turn the baby 180 degrees and relax the attached shoulder by turning it towards the chest, which is easily accessible from the shoulders. Subsequently, the suprapubic pressure is tried to be performed with the mother’s slight strain and gentle pulling of the baby. In some cases, changing the position of the baby is much easier than changing the position of the mother.
 Bu İçeriği Beğendim
Bu İçeriği Beğendim