




 Turkish
Turkish Deutsch
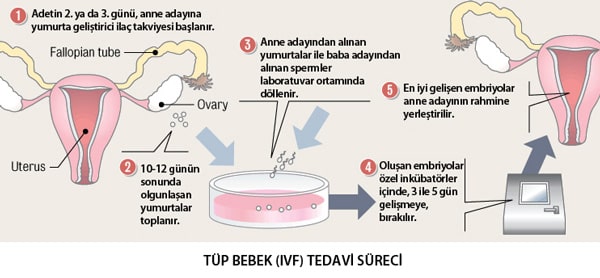
DeutschSteps of IVF Treatment
In cases where the female age is young and the ovarian reserve is sufficient, long protocol, antagonist protocol or Femara protocol can be applied in the presence of congestion in the tubes, male factor or unexplained infertility. There is no significant difference in treatment success between the long protocol and the antagonist protocol.
Due to the risk of hyperstimulation in the presence of polycystic ovaries, the antagonist protocol is chosen because it is a preference that allows precautions to be taken under control of hyperstimulation.
Regardless of which protocol is chosen in cases with low ovarian reserve, treatment success will not change much. Here the resource in the ovary is limited, and the choice of protocol cannot change this fact. However, in these cases, short, antagonist protocols, Femara protocol, natural and modified natural cycles are used more frequently. The most important advantage is the time advantage due to their short duration, and if failure occurs, it will allow retry again in a shorter time.
Application
Basically, in practice, egg activating hormones (FSH, LH or combined) are applied daily under the skin or intramuscularly, and the woman is called for ultrasonography follow-up at 2-4 day intervals. Egg development is monitored regularly and when the eggs reach a sufficient size, an injection of HCG is made under the skin to mature. With this injection, 36 hours later, general anaesthesia, and rarely, local anaesthesia and ultrasonography-guided egg collection is performed.
In embryology laboratory, mature eggs are selected and sperms are placed into the eggs by microinjection. In appropriate environments, fertilization and division is expected. On the day of egg collection, progesterone vaginal gel is started for the preparation of intrauterine tissue for pregnancy. Embryo transfer is performed under ultrasonography 2-5 days after the egg is collected according to the condition of the embryos.
Pregnancy test is done 10-12 days after embryo transfer.
The number of embryos to be transferred is determined by age and the number of applications. According to the rules set by law in our country, a single embryo transfer under the age of 35 is mandatory. In women under 35, two embryos can be transferred in the third application after two unsuccessful attempts. In women over 35, two embryo transfers can be performed directly according to the couple’s preference.
Success rates in IVF applications are inversely proportional to female age. Success rates decrease as women age increases. Cumulative pregnancy rate is 80% in three trials in women under 39 years of age with good ovarian reserve. In other words, 80 out of every 100 couples treated at the end of three attempts at the latest become pregnant.
In women over the age of 39, the cumulative pregnancy rates after three attempts are between 10-30% due to both the number of eggs and the deterioration of the quality of the remaining eggs.
 Bu İçeriği Beğendim
Bu İçeriği Beğendim